Is There a Blood Test for Colon Cancer Runs in My Family
What is colorectal cancer?
Colorectal cancer (cancer that develops in the colon and/or the rectum) is a disease in which abnormal cells in the colon or rectum carve up uncontrollably, ultimately forming a malignant tumor.
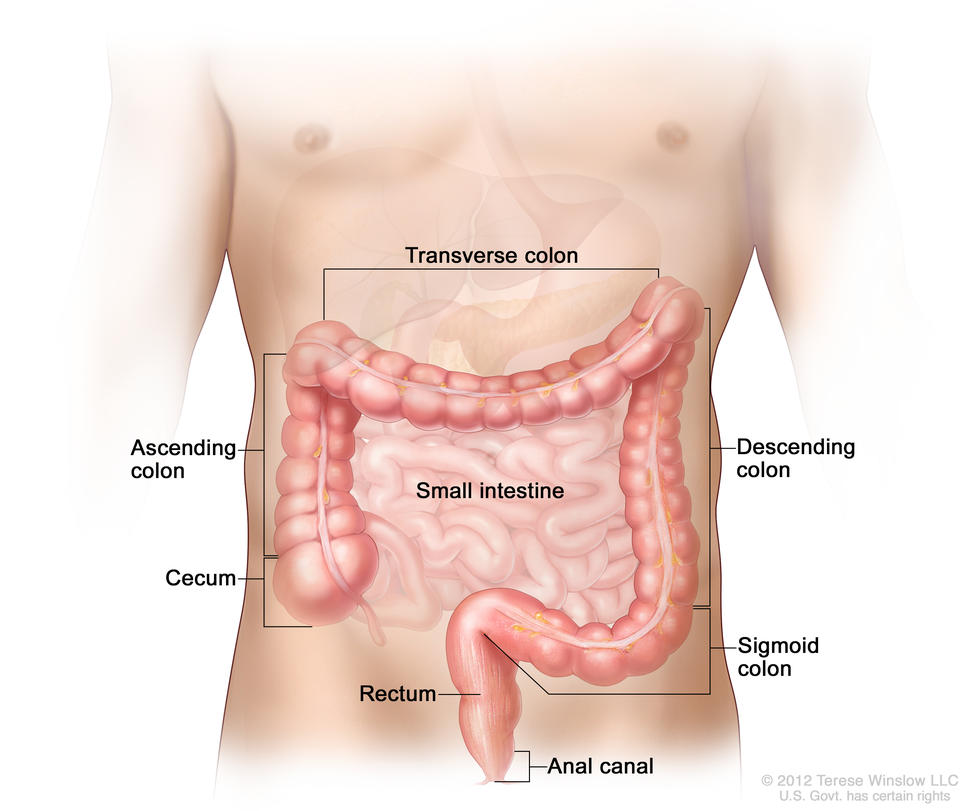
Parts of the colon. Drawing of the forepart of the belly that shows the iv sections of the colon: the ascending colon, the transverse colon, the descending colon, and the sigmoid colon. Also shown are the minor intestine, the cecum, and the rectum. The cecum, colon, rectum, and anal canal make upwardly the big intestine. The cecum, ascending colon, and transverse colon make up the upper, or proximal, colon; the descending colon and sigmoid colon make up the lower, or distal, colon.
Most colorectal cancers begin every bit a growth, or lesion, in the tissue that lines the inner surface of the colon or rectum. Lesions may appear as raised polyps, or, less commonly, they may appear apartment or slightly indented. Raised polyps may be attached to the inner surface of the colon or rectum with a stalk (pedunculated polyps), or they may abound along the surface without a stalk (sessile polyps).
Colorectal polyps are common in people older than l years of age, and nearly do not go cancer. Still, a certain type of polyp known as an adenoma is more likely to become a cancer.
Colorectal cancer is the 3rd most common type of non-peel cancer in both men (after prostate cancer and lung cancer) and women (subsequently breast cancer and lung cancer). It is the second leading cause of cancer death in the United states after lung cancer. In 2021, an estimated 149,500 people in the United States will be diagnosed with colorectal cancer and 52,980 people volition dice from it (i).
Who is at risk for colorectal cancer?
In the United States, colorectal cancer is most common in adults aged 65 to 74. Rates of new colorectal cancer cases are decreasing among adults aged 50 years or older due to an increase in screening and to changes in some hazard factors (for instance, a turn down in smoking) (2). Even so, incidence is increasing amongst younger adults (2 – iv) for reasons that are non known.
An analysis of US population-based cancer registry information from NCI's Surveillance, Epidemiology, and Terminate Results (SEER) program for 2000 to 2014 shows that, each year over this period, the incidence of colorectal cancer increased ii.7% among 20- to 39-year-olds and i.7% among forty- to 49-yr-olds while decreasing 0.5% among l- to 59-yr-olds, 3.3% amongst 60- to 69-year-olds, and iii.eight% among seventy- to 79-year-olds (5).
Although the percentage increases were college in the younger age groups than the older historic period groups, fewer colorectal cancers were still diagnosed in younger people than older people (for example, for 2000 to 2014, 22.5 colorectal cancers were diagnosed per 100,000 people aged 40 to 49 years, compared with 128.6 colorectal cancers diagnosed per 100,000 people aged sixty to 69 years).
The major gamble factors for colorectal cancer are older historic period and having sure inherited weather condition (such as Lynch syndrome and familial adenomatous polyposis), but several other factors have as well been associated with increased risk, including a family history of the disease, excessive alcohol use, obesity, being physically inactive, cigarette smoking, and, mayhap, nutrition.
In addition, people with a history of inflammatory bowel disease (such equally ulcerative colitis or Crohn disease) have a higher risk of colorectal cancer than people without such weather condition.
What methods are used to screen people for colorectal cancer?
Several screening tests have been developed to help doctors find colorectal cancer before symptoms begin, when it may be more treatable. Some tests also permit adenomas and polyps to be removed before they become cancer. That is, colorectal cancer screening may be a form of cancer prevention in addition to early on detection.
The U.s. Preventive Services Task Force (USPSTF) considers the following methods to exist acceptable screening tests for colorectal cancer:
- Stool tests. Both polyps and colorectal cancers tin bleed, and stool tests cheque for tiny amounts of blood in carrion (stool) that cannot exist seen visually. (Blood in stool may also indicate the presence of weather that are not cancer, such every bit hemorrhoids.)
Currently, 3 types of stool tests are approved by the Us Food and Drug Administration (FDA) to screen for colorectal cancer: guaiac FOBT (gFOBT); the fecal immunochemical (or immunohistochemical) exam (FIT, besides known as iFOBT); and multitargeted stool Dna testing (also known every bit FIT-DNA). With these tests, stool samples are collected by the patient using a kit, and the samples are returned to the doctor. People who have a positive finding with these tests are advised to have a colonoscopy.
- gFOBT uses a chemical to discover heme, a component of the claret protein hemoglobin. Because gFOBT can likewise detect heme in some foods (for example, ruddy meat), people must avoid sure foods earlier having this exam.
- FIT uses antibodies to detect hemoglobin protein specifically (5, half-dozen). Dietary restrictions are typically not required for FIT.
- FIT-DNA detects hemoglobin, along with certain DNA biomarkers. The DNA comes from cells in the lining of the colon and rectum that are shed and collect in stool as it passes through the large intestine and rectum.
In one study of people who were at average risk of developing colon cancer and had no symptoms of colon bug (11), the FIT-DNA exam was more sensitive than the FIT test. Notwithstanding, the FIT-DNA examination also was more than likely to identify an abnormality when none was actually nowadays (that is, it had more imitation-positive results, which can lead to unnecessary colonoscopies). Experts more often than not suggest FIT-DNA testing at least every 3 years (half dozen).
- Sigmoidoscopy. In this exam, the rectum and sigmoid colon are examined using a sigmoidoscope, a flexible lighted tube with a lens for viewing and a tool for removing tissue. This instrument is inserted through the anus into the rectum and sigmoid colon as air is pumped into the colon to expand it so the doctor can see the colon lining more than clearly. During sigmoidoscopy, abnormal growths in the rectum and sigmoid colon can exist removed for assay (biopsied). The lower colon must be cleared of stool before sigmoidoscopy, but the preparation is non very all-encompassing. People are usually non sedated for this test.
Clinical trials accept shown that having sigmoidoscopy lowers the risks of developing and dying from colorectal cancer (12–16). Experts generally recommend sigmoidoscopy every 5 or 10 years for people at average risk who take had a negative exam consequence (ten). People who are screened with sigmoidoscopy may also be tested every few years with FIT.
- Colonoscopy. In this test, the rectum and entire colon are examined using a colonoscope, a flexible lighted tube with a lens for viewing and a tool for removing tissue. Like the shorter sigmoidoscope, the colonoscope is inserted through the anus into the rectum and the colon as air is pumped into the colon to expand it and then the physician can see the colon lining more conspicuously. During colonoscopy, whatever abnormal growths in the unabridged colon and the rectum can be removed. The preparation for colonoscopy requires a thorough cleansing of the entire colon before the test. Nearly patients receive some class of sedation during the exam.
A meta-analysis of six observational studies reported that screening with colonoscopy substantially reduces the risks of developing and dying from colorectal cancer (17). Experts recommend colonoscopy every 10 years for people at average risk equally long equally their examination results are negative.
Virtual colonoscopy, also chosen computed tomographic (CT) colonography, is a screening method that uses special 10-ray equipment (a CT scanner) to produce a series of pictures of the colon and the rectum from outside the body. A computer then assembles these pictures into detailed images that tin can testify polyps and other abnormalities. Equally with standard colonoscopy, a thorough cleansing of the colon is necessary earlier this test. If polyps or other aberrant growths are constitute during a virtual colonoscopy, a standard colonoscopy must usually exist performed to remove them.
Considering virtual colonoscopy too produces images of areas exterior the colon and rectum it can pb to the unintentional discovery of medical findings in these areas that require additional follow-upwardly procedures. Virtual colonoscopy may besides miss small polyps (18). However, many small-scale polyps may not be likely to become cancer and so taking them out may not be of benefit.
- Other methods. Several other tests to screen for colorectal cancer exist, although these are not generally recommended.
Blood-based Dna test (liquid biopsy). A blood exam for an altered gene called SEPT9 is FDA approved to be used to screen adults 50 years or older at boilerplate risk for colorectal cancer who take been offered and have a history of not completing colorectal cancer screening. At that place is no show yet that this test can reduce deaths from colorectal cancer.
Double-dissimilarity barium enema (DCBE). This test is another method of visualizing the colon from outside the body. In DCBE, a serial of x-ray images of the entire colon and rectum is taken later on the patient is given an enema with a barium solution. The barium helps to outline the colon and the rectum on the images. DCBE is rarely used for colorectal cancer screening; nonetheless, information technology may exist used for people who cannot undergo standard colonoscopy—for example, because they are at particular risk for complications.
Single-specimen gFOBT washed in a doctor's part. Doctors sometimes perform a single-specimen gFOBT on a stool sample nerveless during a digital rectal exam as part of a routine physical test. However, this approach has not been shown to be an constructive way to screen for colorectal cancer (19).
What practice colorectal cancer screening guidelines say about who should accept colorectal cancer screening?
Expert medical groups, including the US Preventive Services Task Force (USPSTF) (6), strongly recommend screening for colorectal cancer. Although some details of the recommendations vary, most groups now generally recommend that people at average risk of colorectal cancer become screened at regular intervals beginning at age 45 or 50 (half-dozen, ten, 20–22).
The proficient medical groups generally recommend that screening continue to age 75; for those aged 76 to 85 years, the decision to screen is based on the private's life expectancy, health atmospheric condition, and prior screening results.
People who are at increased risk of colorectal cancer because of a family history of colorectal cancer or documented advanced polyps or because they have inflammatory bowel affliction or certain inherited weather condition (such as Lynch syndrome and familial adenomatous polyposis) may be advised to start screening earlier and/or take more frequent screening.
How can people and their health care providers decide which colorectal cancer screening exam(s) to use?
It is important to have colorectal cancer screening. Different tests accept different advantages and disadvantages, and people should talk with their health intendance provider virtually which exam is best for them.
An private's decision about which test to have may depend on:
- the person's historic period, medical history, family history, and general health
- potential harms of the test
- the grooming required for the test
- whether sedation may be needed for the test
- the follow-up care needed after the test
- the convenience of the examination
- the price of the test and the availability of insurance coverage
The table beneath summarizes central features of the different colorectal screening tests that people may want to consider when choosing a test.
| Test | Nutrition and medication changes before test? | Invasive procedure? | Grooming (colon cleansing) needed? | Sedation needed? | Test frequency | Boosted considerations |
|---|---|---|---|---|---|---|
| Stool tests | Yes for gFOBT, no for FIT or FIT-Deoxyribonucleic acid | No | No | No | Every year to every 3 years, depending on the test |
|
| Sigmoidoscopy | Yes | Yes | Yes (less extensive than for colonoscopy) | Unremarkably no | Every v to 10 years, peradventure with more than frequent FIT |
|
| Colonoscopy | Yep | Yes | Yes | Yes | Every 10 years |
|
| Virtual colonoscopy | No | No | Yes | No | Every 5 years |
|
Does health insurance pay for colorectal cancer screening?
Colorectal cancer screening is a preventive service that the Health Insurance Marketplace and many other health plans are required to cover. Medicare covers several colorectal cancer screening tests for its beneficiaries. All the same, Medicare and some insurance companies currently exercise not pay for the costs of virtual colonoscopy. Specific information about Medicare benefits for colorectal cancer screening is bachelor on the Medicare website.
A colonoscopy to follow upward on a screening test with a positive result, such as an abnormal stool examination or fifty-fifty a lesion detected on a screening colonoscopy, is considered to be a diagnostic exam and may not be covered (or not covered equally fully as a screening colonoscopy). Some insurers consider a screening colonoscopy that reveals a polyp that must be removed to be a diagnostic test and charge accordingly. People should check with their wellness insurance provider to decide their colorectal cancer screening coverage and what their out-of-pocket expenses may be if the exam finds an abnormality that needs to exist followed upward.
What happens if a colorectal cancer screening test finds an abnormality?
If a screening exam finds an abnormality (a lesion or tumor), additional tests may be needed. These tests most oftentimes include a colonoscopy if it has not already been washed, such as in the case of stool blood testing. If an aberration is found during sigmoidoscopy, a biopsy or polypectomy may be performed during the test, and a follow-up colonoscopy may be recommended. If an abnormality is found during a standard colonoscopy, a biopsy or polypectomy may be performed during the test to make up one's mind whether cancer is nowadays. If an abnormality is detected during virtual colonoscopy, the patient will be referred for a standard colonoscopy.
What new tests are existence adult for colorectal cancer screening?
Amid new approaches to colorectal cancer screening that are existence explored are means to improve visualization of the colon. One technique is sheathing colonoscopy (too called capsule endoscopy), in which a person swallows a pill-like capsule that contains a tiny wireless photographic camera. The camera takes pictures of the inside of the digestive tract and sends them to a small recorder that is worn on the patient's waist or shoulder. The pictures are and then viewed on a computer by the doctor to check for signs of disease. The capsule passes out of the body during a bowel movement. Cleansing of the colon is still necessary earlier this test. This method is currently approved for patients with an incomplete colonoscopy and for detection of colon polyps in patients with bear witness of lower GI bleeding merely not every bit a stand up-lonely screening examination.
One new arroyo to colorectal cancer screening is to look for cells released by colorectal polyps and tumors into the bloodstream (24). These so-called circulating tumor cells (CTCs) are rare, however. Researchers have developed an ultrasensitive antibody-linked CTC detection applied science to capture colorectal epithelial cells associated with colorectal tumors and adenomas in blood samples (25). In a proof-of-concept study, this blood-based CTC exam was able to distinguish between patients with colorectal adenomas or cancer and people without cancer (26).
Researchers have also identified modest molecules, chosen metabolites, in urine that may signal the presence of colorectal polyps and tumors (27, 28). In a clinical written report, a metabolomic-based urine test was better able to identify patients with adenomas than stool-based tests (29).
Researchers are also trying to meliorate the sensitivity of stool-based screening for detecting advanced adenomatous polyps, which can potentially become colorectal cancer, past testing for the presence of multiple biomarkers. For example, measuring three poly peptide biomarkers in stool—hemoglobin, calprotectin, and serpin family F member ii—improved the ability of FIT to detect advanced lesions (including colorectal cancer) by 35% without reducing its specificity (30).
Information about ongoing clinical trials that are studying methods for colorectal cancer screening tin be institute in NCI's clinical trials database. You may also contact NCI'southward Cancer Information Service at one-800-iv-CANCER (i-800-422-6237) for assistance with searching the clinical trials database.
Source: https://www.cancer.gov/types/colorectal/screening-fact-sheet
0 Response to "Is There a Blood Test for Colon Cancer Runs in My Family"
Post a Comment